Retina & Vitreous
Retinal
Care
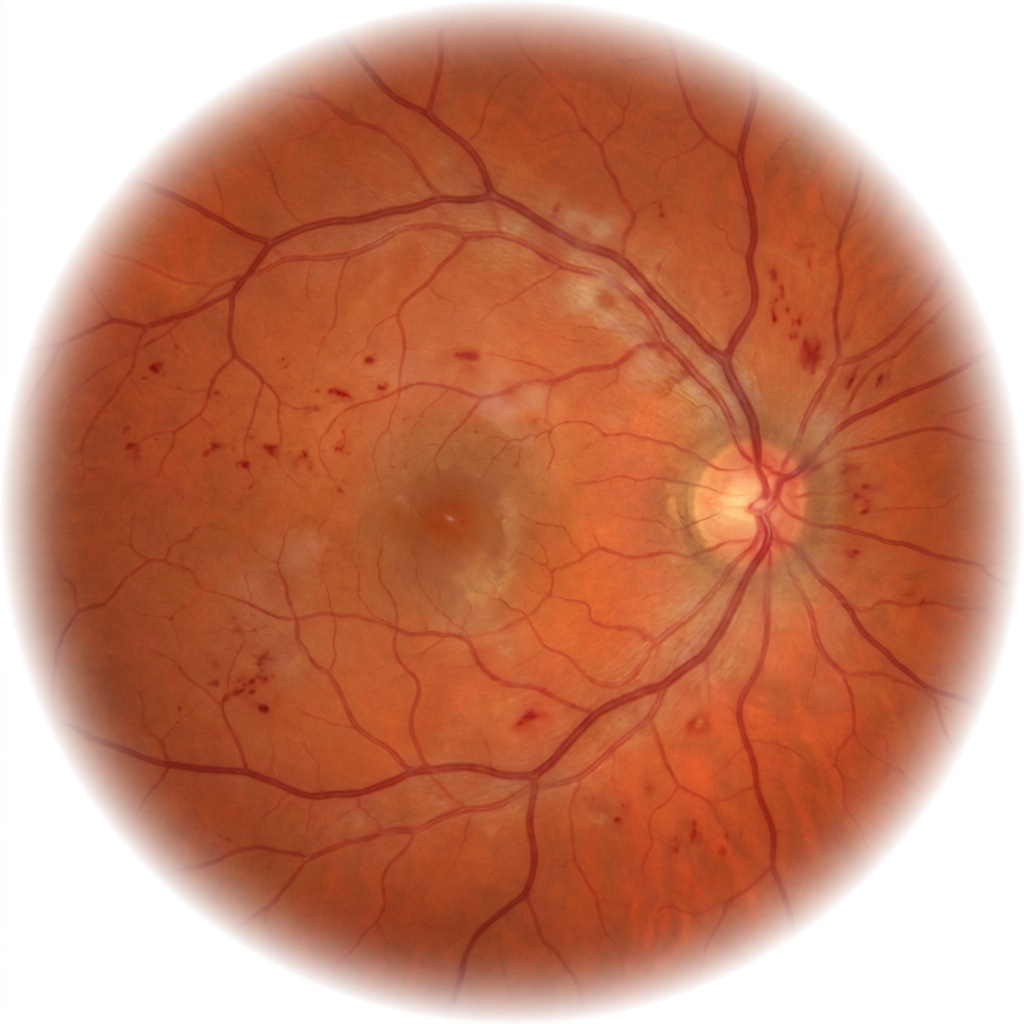
The retina is the camera film of the eye — once it is damaged, vision lost cannot be recovered. Anti-VEGF injections, retinal laser, and vitreoretinal surgery can halt progression and, in many cases, restore significant sight.
Anti-VEGFGold-standard for wet AMD & DR
OCT-AAngiography — no dye
MonthlyMonitoring for diabetics

Same-week injectionUrgent anti-VEGF slots available