Diabetic Retinopathy Prevention
Diabetic Eye
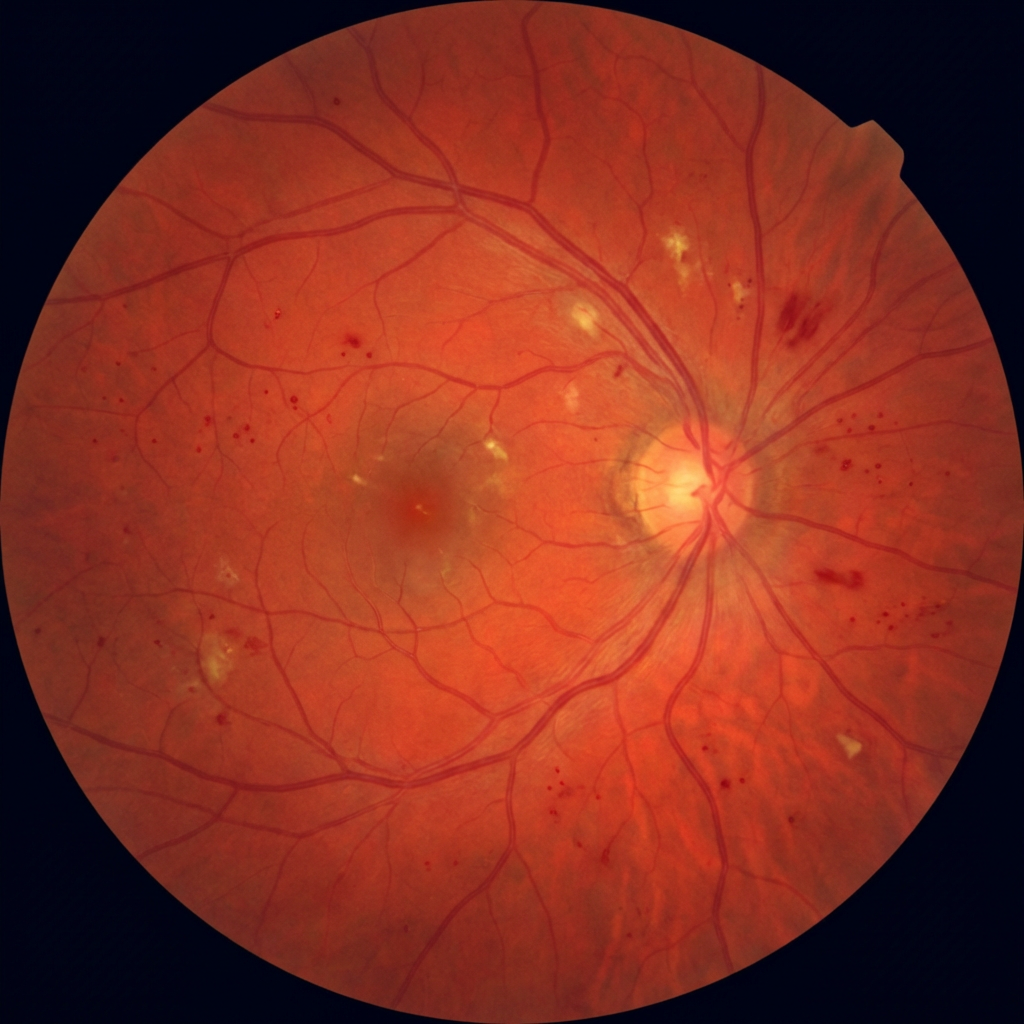
Screening
90% of diabetic blindness is preventable with annual screening and timely treatment. Diabetic retinopathy causes no symptoms until it is advanced — by the time your vision blurs, significant and often irreversible damage has already occurred.
1 in 3Diabetics develop retinopathy
AnnualScreening — every diabetic
90%Blindness is preventable

₹800Annual diabetic eye screen