Medical Dermatology
Fungal & Nail
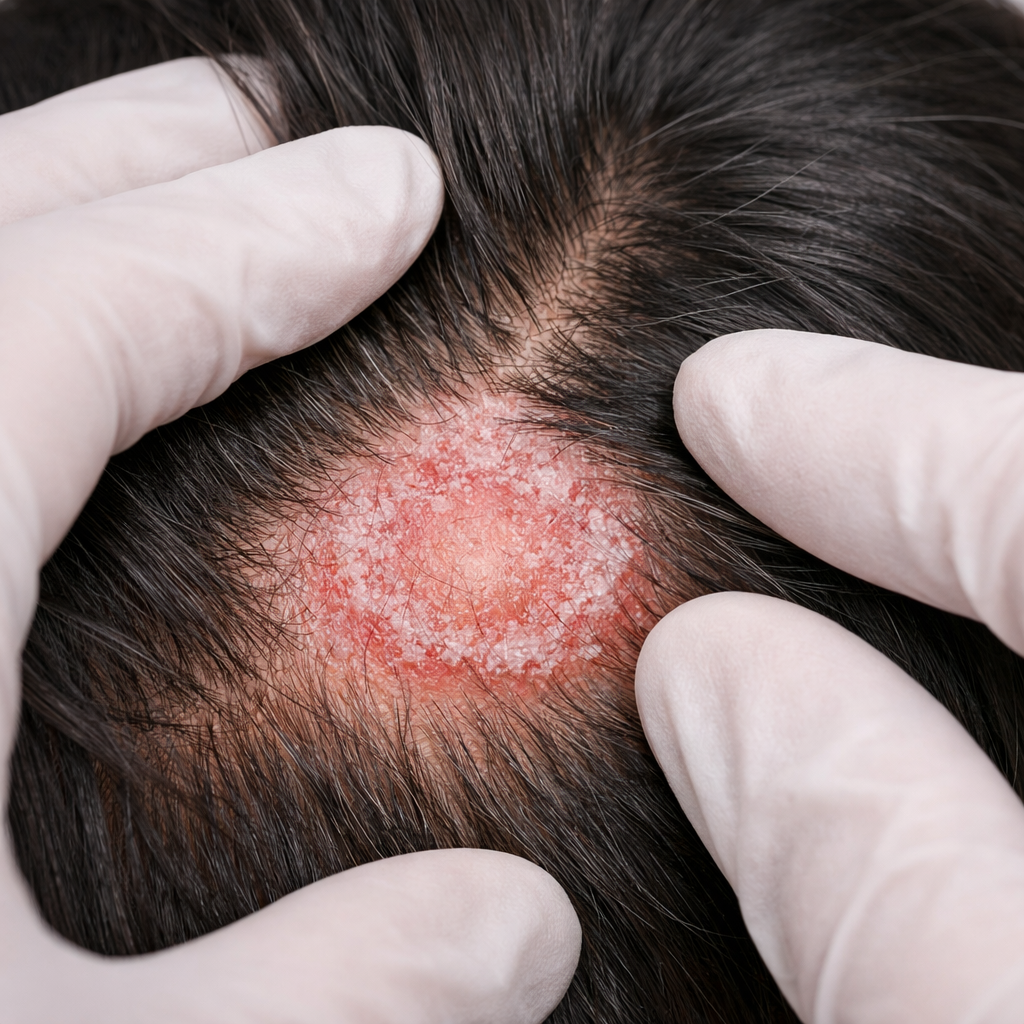
Infections
Ringworm that keeps returning, nails that won't clear, athlete's foot resistant to pharmacy creams — the answer is accurate KOH microscopy diagnosis first, then the right antifungal at the correct dose for the right duration.
KOHMicroscopy on-site
NailOnychomycosis treated
AllTinea types managed

₹500Starting consultation
.png)