Glaucoma Care
Glaucoma
Management
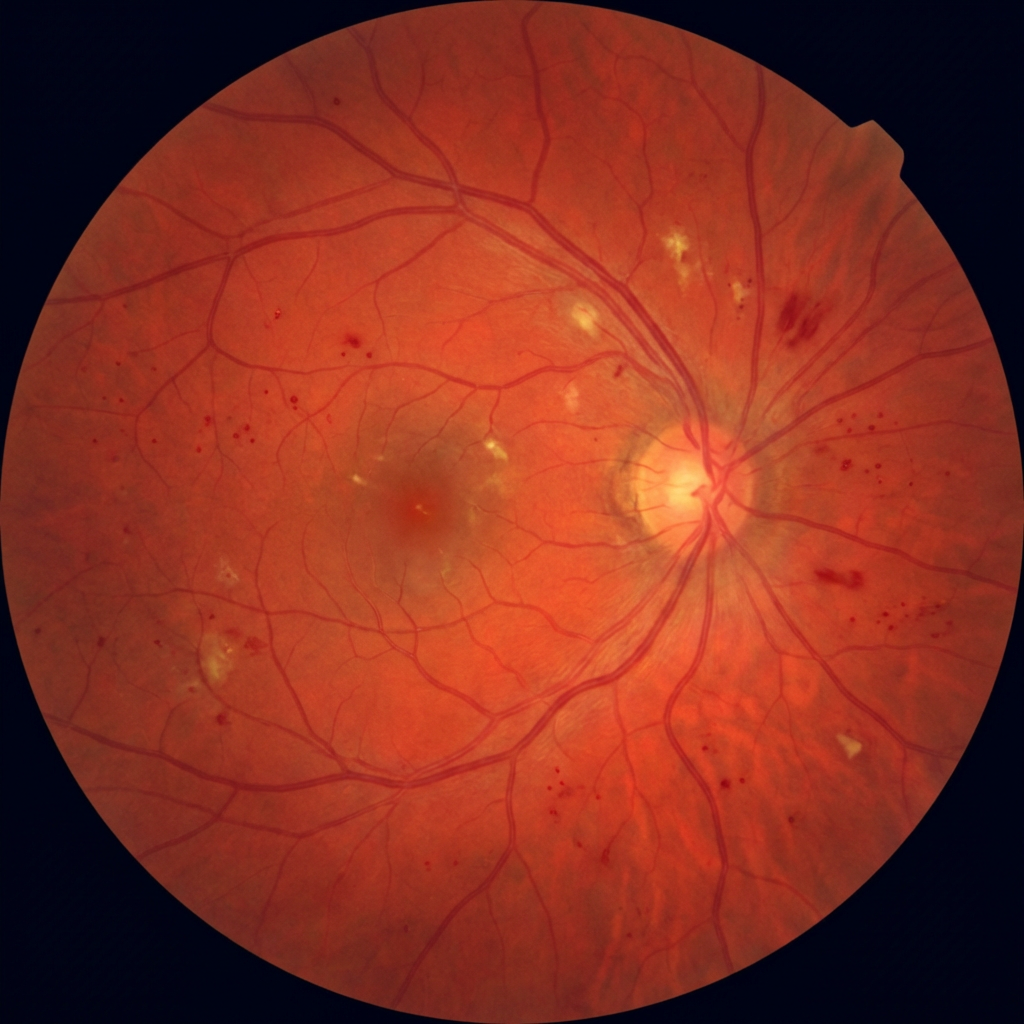
The "silent thief of sight" causes irreversible vision loss before you notice a single symptom. Early detection with OCT and visual field analysis — combined with targeted treatment — is the only way to preserve your vision for life.
0Symptoms in early stages
OCTNerve fibre imaging
SLTLaser — 5 min procedure

Annual screeningCritical for over-40s & diabetics